

The accurate targeting of tumours with maximal sparing of normal tissues has always been the foremost goal of radiotherapy practice. Over the past two decades, the ability to achieve this goal has improved greatly through advances in imaging technology, specifically the development of hybrid imaging supported with Computerized Tomography (CT), Magnetic Resonance Imaging (MRI), Positron Emission Tomography (PET), Single-Photon Emission Computed Tomography, Single Photon Emission Computed Tomography (SPECT), and Fusion PET/CT.  Recent years have seen an increasing trend in the use of PET and PET/CT. Along with diagnosis, staging, relapse detection and follow-up, one of the main applications of PET/CT is the assessment of treatment response and treatment planning. PET provides molecular information about the tumour microenvironment (‘Functional imaging’) in addition to anatomical imaging. Therefore, it is highly beneficial to integrate PET data into radiotherapy treatment planning.
Recent years have seen an increasing trend in the use of PET and PET/CT. Along with diagnosis, staging, relapse detection and follow-up, one of the main applications of PET/CT is the assessment of treatment response and treatment planning. PET provides molecular information about the tumour microenvironment (‘Functional imaging’) in addition to anatomical imaging. Therefore, it is highly beneficial to integrate PET data into radiotherapy treatment planning.
The use of functional imaging to better delineate the treatment target is a good example of individualized treatment. In fact, instead of using a previously established field or set of fields, the radiation dose is shaped on the tumour for each individual patient. PET/CT radiotherapy treatment planning is an evolving strategy, which presents some obstacles that need to be addressed. The use of PET for target volume delineation requires specific tuning of parameters such as image acquisition, processing and segmentation and these may vary from one tumour site to another. This is currently the topic of intensive research work.
Fortunately, developments in imaging technology coupled with advances in computer technology have fundamentally changed the processes of tumour targeting and radiation therapy planning. The ability to display anatomical information in an infinite selection of views has led to the emergence of three-dimensional conformal radiotherapy (3D–CRT); a modality in which the volume treated conforms closely to the shape of the tumour volume.
While several new technological developments emerged in the field of radiation oncology in 2009, the following two important issues were highlighted during the International Conference on Advances in Radiation Oncology. The International Atomic Energy Agency (IAEA) sponsored this conference:
- The first important issue concerns efforts to assess the comparative value of cobalt units versus linear accelerators, focusing on which is of particular importance to low and middle income countries. In a comparative assessment of nuclear technologies in the human health field carried out by the IAEA, experts agreed that the choice between these two treatment modalities will depend on several factors including the availability of national cancer control plans, the existence of a required critical mass of qualified scientific and medical staff, as well as the availability of adequate infrastructure; and
- Secondly, issues of uncertainty and accuracy in radiation oncology are becoming more important globally as treatment techniques become more sophisticated, with higher doses being used to improve cancer cure rates. There is an increased appreciation that quality assurance activities and accurate documentation are required at each step of the patient management path. The development of evidence-based clinical guidelines and protocols is being encouraged.
 During the past decade, the leap in radiotherapy technology has been overwhelming. Here are some major highlights of recent technological advances in radiation oncology:
During the past decade, the leap in radiotherapy technology has been overwhelming. Here are some major highlights of recent technological advances in radiation oncology:
1. MAJOR HIGHLIGHTS OF RECENT TECHNOLOGICAL ADVANCES:
1.1 Intensity Modulated Radiation Therapy:
This therapy is a sophisticated type of three-dimensional conformal radiotherapy that assigns non-uniform intensities to a tiny subdivision of beams called beamlets. The ability to manipulate the intensities optimally of individual rays within each beam, leads to greatly increased control over the overall radiation fluency. For instance, the total number of photons/particles crossing over a given volume per unit time. This in turn allows for the custom design of optimal dose distributions. Improved dose distributions often lead to improved tumour control and reduced toxicity in normal tissue.
When a tumour is not separated from the surrounding organs at risk and/or has a concave or irregular shape, there may be no practical combination of uniform-intensity beams that will safely treat the tumour and spare the healthy organs. In such instances, adding IMRT to beam shaping allows for much tighter conformity to targets. IMRT requires the setting of the relative intensities of tens of thousands of individual beamlets comprising an intensity modulated treatment plan. This task cannot be accomplished manually, it requires the use of a Multileaf Collimator (MLC), and specialized computer assisted optimization methods.
There is still a lack of randomized trials that clearly demonstrate the clinical benefits of IMRT in many tumour sites other than improved dose distribution and a reduction in toxicity in some situations. Unexpected toxicities and recurrences have been reported in specialized literature on radiation oncology.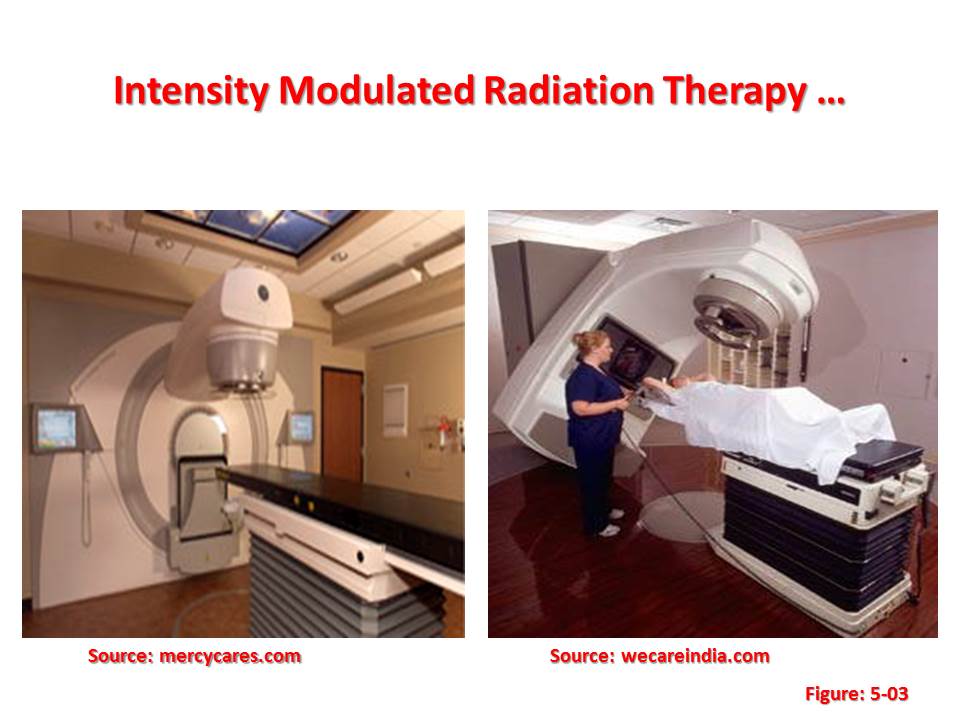 Advanced radiation treatment technologies such as IMRT require improved patient immobilization and image guidance techniques. There is some debate as to whether image guidance is always required with IMRT to ensure accurate delivery and whether it is required daily. This is due to the use of tighter margins around the tumour and the sharp dose fall-off with IMRT. Image guidance may be necessary in specific cases, such as when immobilization is not optimal or when hypofractionation is used. Other techniques to control organ motion during treatment such as respiratory-gating and breath-hold techniques may be necessary when reduced target volumes are considered.
Advanced radiation treatment technologies such as IMRT require improved patient immobilization and image guidance techniques. There is some debate as to whether image guidance is always required with IMRT to ensure accurate delivery and whether it is required daily. This is due to the use of tighter margins around the tumour and the sharp dose fall-off with IMRT. Image guidance may be necessary in specific cases, such as when immobilization is not optimal or when hypofractionation is used. Other techniques to control organ motion during treatment such as respiratory-gating and breath-hold techniques may be necessary when reduced target volumes are considered.
Since IMRT sometimes uses more treatment fields from different directions, its use may increase the volume of normal tissue receiving low doses that might lead to a higher risk of secondary cancers. This is of particular concern in the case of paediatric patients. With the introduction of any advanced technology, such as IMRT and image guided radiation therapy, data should be collected in advance to allow a thorough evaluation of cost-effectiveness and cost-benefit.
Experts advise caution in the widespread implementation of these new technologies. If the identification of target tissues is uncertain when margins around target volumes are tight, the likelihood of geographical misses or under dosing of the target increases.
1.2 Image Guided Radiation Therapy:
Image Guided Radiation Therapy (IGRT) is the use of frequent imaging during a course of radiation therapy to improve the precision and accuracy of the delivery of treatment.
In IGRT, machines that deliver radiation, such as a linear accelerator, are equipped with imaging technology so that the physician can image the tumour immediately before or even during the time radiation is delivered, while the patient is positioned on the treatment table. Using specialized computer software, these images are then compared to the images taken during simulation. Any necessary adjustments are then made to the patient’s position and/or radiation beams in order to more precisely target radiation at the tumour and avoid healthy surrounding tissue.
IGRT is used to treat tumours in areas of the body that are prone to movement, such as the lungs (affected by breathing), liver, and prostate gland, as well tumours located close to critical organs and tissues. It is often used in conjunction with intensity-modulated radiation therapy (IMRT) or stereotactic body radiotherapy (SBRT), advanced modes of high-precision radiotherapy that utilize computer-controlled x-ray accelerators to deliver precise radiation doses to a malignant tumour or specific areas within the tumour. 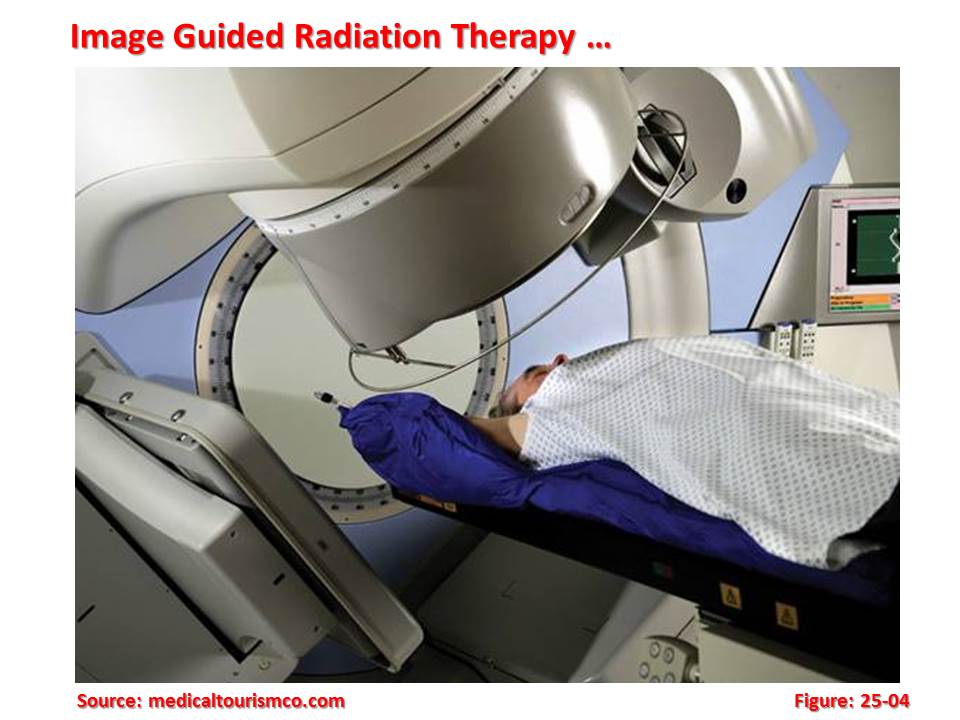 Safety margins are used in order to account for geometric uncertainties during radiotherapy (patient movements, internal organ movements). In many cases, these margins include part of the organs at risk, thereby limiting dose increases. The aim of image guided radiation therapy is to improve accuracy by imaging tumours and critical structures just before irradiation.
Safety margins are used in order to account for geometric uncertainties during radiotherapy (patient movements, internal organ movements). In many cases, these margins include part of the organs at risk, thereby limiting dose increases. The aim of image guided radiation therapy is to improve accuracy by imaging tumours and critical structures just before irradiation.
In IGRT, imaging equipment is mounted on or built into the machine that delivers radiation, such as a linear accelerator. Imaging equipment may also be mounted in the treatment room. Imaging technologies used in IGRT include x-rays, computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), and ultrasound (US).
Imaging performed prior to or during radiation therapy sessions is painless. Side effects of radiation treatment include problems that occur because of the treatment itself as well as from radiation damage to healthy cells in the treatment area.
Radiation therapy can cause early and late side effects. Early side effects occur during or immediately after treatment and are typically gone within a few weeks. Common early side effects of radiation therapy include tiredness or fatigue and skin problems. Skin in the treatment area may become more sensitive, red, irritated, or swollen. Other skin changes include dryness, itching, peeling and blistering.
The availability of high quality imaging systems and automatic image registration has led to many new clinical applications such as the high precision hypofractionated treatments of brain metastases and solitary lung tumours with real time tumour position corrections.
1.3 Helical Tomo Therapy:
Patients with brain tumours at risk for dissemination through the cerebrospinal fluid often require craniospinal axis irradiation. Comprehensive irradiation of the craniospinal space is technically demanding. Craniospinal radiation typically utilizes prone positioning of the patient combined with careful junctioning between opposed lateral cranial fields and a posterior spine field. In larger patients, an additional junction between upper and lower spine fields may be required. Periodic junction shifts are introduced throughout the treatments to address the potential risk of underdose or overdose at the field junctions. Many of the patients requiring craniospinal radiotherapy are paediatric patients who may have difficulty cooperating with prone positioning for treatment and may require daily anesthesia for treatment. In these cases, supine positioning may be preferable depending on the institution preference. With supine or prone positioning, the challenge of setting and verifying multiple field junctions and the maintenance of a homogeneous dose over a long treatment volume remains.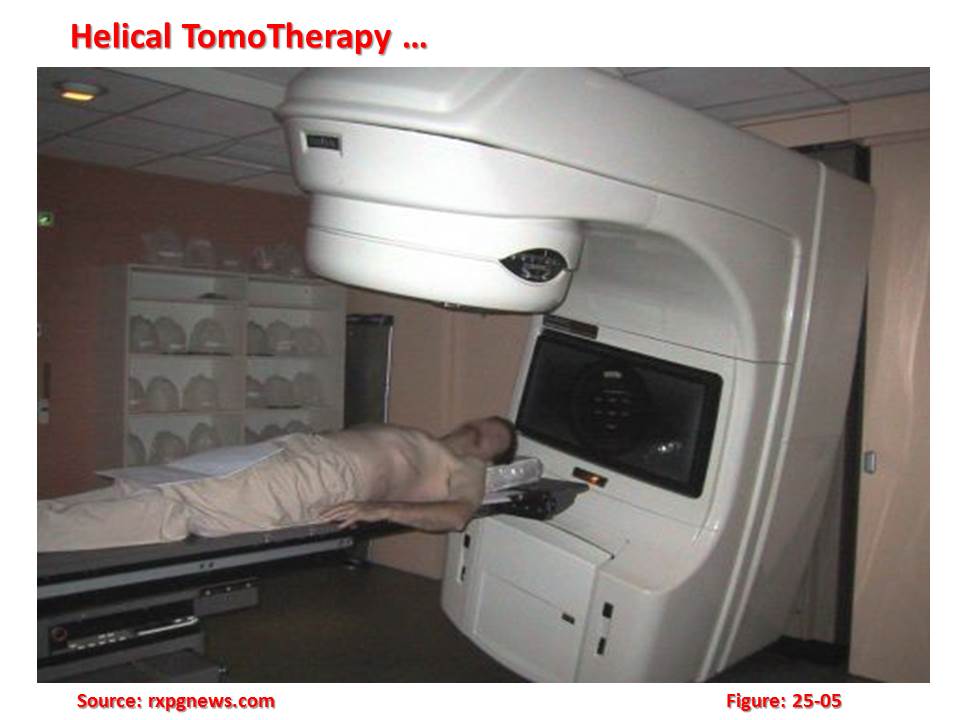 Helical tomotherapy (HT) is a novel approach to the delivery of radiation for cancer treatment. It relies on a six MV linear accelerator mounted on a ring gantry that rotates around the patient as they advance slowly through the ring. During treatment delivery, the radiation fan beam is defined using a 64-leaf collimator. Each leaf projects a shadow of 0.625 mm width at the isocentre 85 cm away from the target and the fan beam width is adjustable from 0.5 cm to 5 cm. The alteration of leaf positions as a function of the gantry position while the patient advances slowly through the gantry allows great flexibility in sculpting a sophisticated target dose distribution while sparing critical normal structures. In addition, the smooth, helical delivery of the intensity-modulated fan beam allows the treatment of extended volumes in the cephalo–caudad direction in either the prone or supine position without the need for junctioning. Experts sought to model the potential advantages of HT delivery for craniospinal radiation for the case of a paediatric patient with disseminated ependymoma.
Helical tomotherapy (HT) is a novel approach to the delivery of radiation for cancer treatment. It relies on a six MV linear accelerator mounted on a ring gantry that rotates around the patient as they advance slowly through the ring. During treatment delivery, the radiation fan beam is defined using a 64-leaf collimator. Each leaf projects a shadow of 0.625 mm width at the isocentre 85 cm away from the target and the fan beam width is adjustable from 0.5 cm to 5 cm. The alteration of leaf positions as a function of the gantry position while the patient advances slowly through the gantry allows great flexibility in sculpting a sophisticated target dose distribution while sparing critical normal structures. In addition, the smooth, helical delivery of the intensity-modulated fan beam allows the treatment of extended volumes in the cephalo–caudad direction in either the prone or supine position without the need for junctioning. Experts sought to model the potential advantages of HT delivery for craniospinal radiation for the case of a paediatric patient with disseminated ependymoma.
Helical tomotherapy is a modality of radiation therapy in which the radiation is delivered slice-by-slice (hence, the use of the Greek prefix tomo-, which means ‘slice’). This method of delivery differs from other forms of external beam radiation therapy in which the entire tumour volume is irradiated at one time. The overall treatment time is relatively short which the main advantage of this method is.
Radiation therapy has developed with a strong reliance on homogeneity of dose throughout the tumour.
Helical tomotherapy embodies the sequential delivery of radiation to different parts of the tumour that raises two important issues. First, this method, known as ‘field matching’, brings with it the possibility of a less-than-perfect match between two adjacent fields with a resultant ‘hot spot’ and/or ‘cold spot’ within the tumour. The second issue is that if the patient or tumour moves during this sequential delivery, a hot or cold spot may result. The first problem can be overcome, or at least minimized, by careful construction of the beam delivery system. The second requires close attention to the position of the target throughout treatment delivery.
1.4 Volumetric Modulated Arc Therapy:
In this therapy, a novel plan optimization platform is presented where treatment is delivered efficiently and accurately in a single dynamically modulated arc. Improvements in patient care achieved through image-guided positioning and plan adaptation have resulted in an increase in overall treatment times.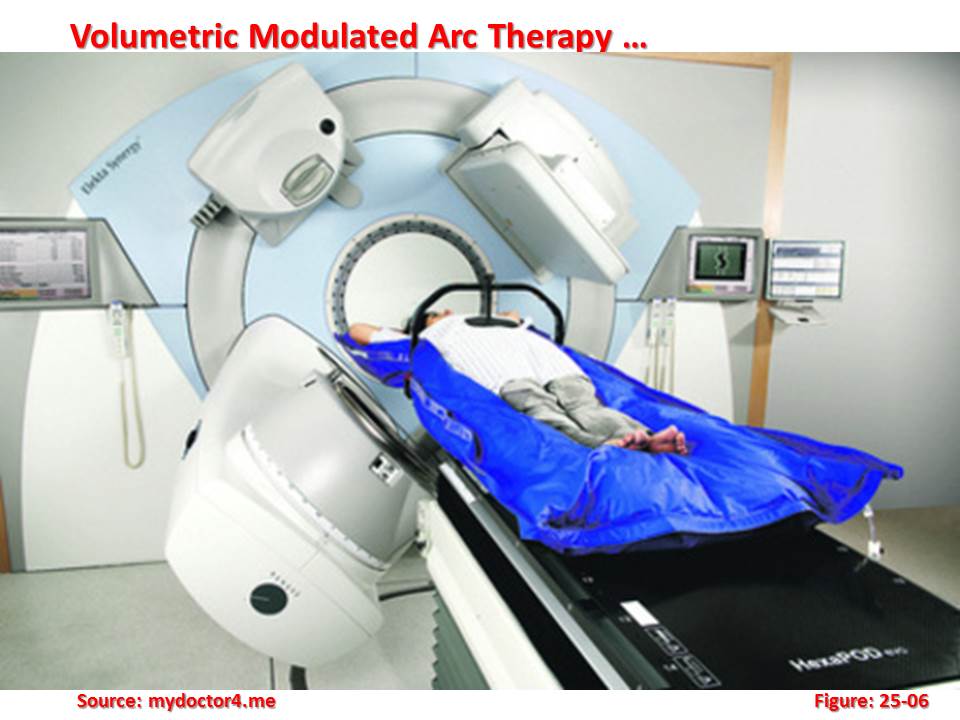 Intensity-modulated radiation therapy (IMRT) has also increased treatment time by requiring a larger number of beam directions, increased monitor units (MU), and, in the case of tomotherapy, a slice-by-slice delivery. In order to maintain a similar level of patient care throughout it will be necessary to increase the efficiency of treatment delivery. The solution proposed here is a novel aperture-based algorithm for treatment plan optimization where dose is delivered during a single gantry arc of up to 360 deg.
Intensity-modulated radiation therapy (IMRT) has also increased treatment time by requiring a larger number of beam directions, increased monitor units (MU), and, in the case of tomotherapy, a slice-by-slice delivery. In order to maintain a similar level of patient care throughout it will be necessary to increase the efficiency of treatment delivery. The solution proposed here is a novel aperture-based algorithm for treatment plan optimization where dose is delivered during a single gantry arc of up to 360 deg.
The technique is similar to tomotherapy in that a full 360 deg of beam directions are available for optimization but is fundamentally different in that the entire dose volume is delivered in a single source rotation. The new technique is referred to as volumetric modulated arc therapy (VMAT). Multileaf collimator (MLC) leaf motion and number of MU per degree of gantry rotation is restricted during the optimization so that gantry rotation speed, leaf translation speed, and dose rate maxima do not excessively limit the delivery efficiency.
During planning, investigators model continuous gantry motion by a coarse sampling of static gantry positions and fluence maps or MLC aperture shapes. The technique presented here is unique in that gantry and MLC position sampling is progressively increased throughout the optimization. Using the full gantry range will theoretically provide increased flexibility in generating highly conformal treatment plans. In practice, the additional flexibility is somewhat negated by the additional constraints placed on the amount of MLC leaf motion between gantry samples.
A series of studies are performed that characterize the relationship between gantry and MLC sampling, dose modeling accuracy, and optimization time. Results show that gantry angle and MLC sample spacing as low as 1 deg and 0.5 cm, respectively, is desirable for accurate dose modeling. It is also shown that reducing the sample spacing dramatically reduces the ability of the optimization to arrive at a solution. The competing benefits of having small and large sample spacing are mutually realized using the progressive sampling technique described here. Preliminary results show that plans generated with VMAT optimization exhibit dose distributions equivalent or superior to static gantry IMRT. Timing studies have shown that the VMAT technique is well suited for on-line verification and adaptation with delivery times that are reduced to approximately 1.5-3 min for a 200-cGy fraction.
1.5 Stereotactic Radiotherapy:
Stereotactic radiotherapy (also called ‘radiosurgery’ although there is no surgery involved) consists of the delivery of a relatively high dose of radiation to a small volume using a precise stereotactic localization technique.
The stereotactic component of the technique refers to the immobilization or fixation of the patient with a rigid head frame system that establishes a patient-specific coordinate system for the entire treatment process. This modality is usually applied in the treatment of intracranial tumours. After placement of the head frame, typically by use of four pins that penetrate the scalp and impinge the outer table of the skull, an imaging study (CT, MRI) is performed to localize the target volume relative to the head frame coordinates.
Stereotactic radiotherapy can be delivered using a gamma knife device. This machine uses 201 small cobalt-60 sources collimated to converge in a small volume where the lesion is located.
A linear accelerator can be modified to perform stereotactic radiotherapy. The linear accelerator is modified to accept a tertiary collimator assembly to accurately position circular collimators to form small circular fields of 4 to 40 mm in diameter. The peripheral dose is spread over a large volume by using radiation paths that follow arcs. Stereotactic radiotherapy is continuously being improved and it remains a popular and increasingly used modality.
Small intracranial tumours in general, pituitary adenomas, small meningiomas, acoustic neuroma, craniopharyngioma, pineal tumours, brain metastasis or non-malignant conditions such as arterio-venous malformations are often treated with stereotactic radiotherapy. Stereotactic body radiotherapy is also being used to treat localized liver tumours.
1.6 Robotic Radiotherapy:
Robotic radiotherapy is a frameless robotic radiosurgery system. The two main elements of robotic radiotherapy are the radiation produced from a small linear accelerator and a robotic arm that allows the energy to be directed towards any part of the body from any direction.
The robotic radiotherapy system is a method of delivering radiotherapy with the intention of targeting treatment more accurately than standard radiotherapy. Owing to its high cost, it is not widely available, although the number of centres offering the treatment around the world has grown in recent years to over 150, particularly in North America, East Asia and Europe. The robotic radiotherapy system is used for treatment of malignant and benign tumours, as well as other medical conditions.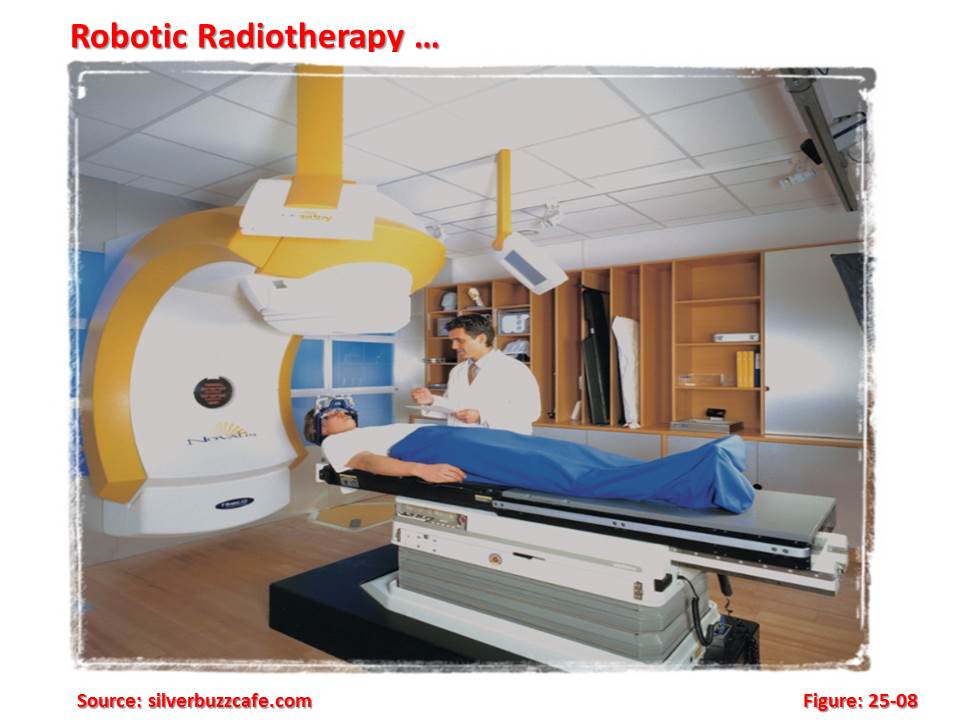 1.7 Particle Therapy:
1.7 Particle Therapy:
There is new hope for patients with inoperable tumours. A new treatment developed by Siemens in conjunction with the GSI Society for Heavy Ion Research shows promise. Based on irradiation with fast particles, the therapy destroys tumours permanently with minimum trauma.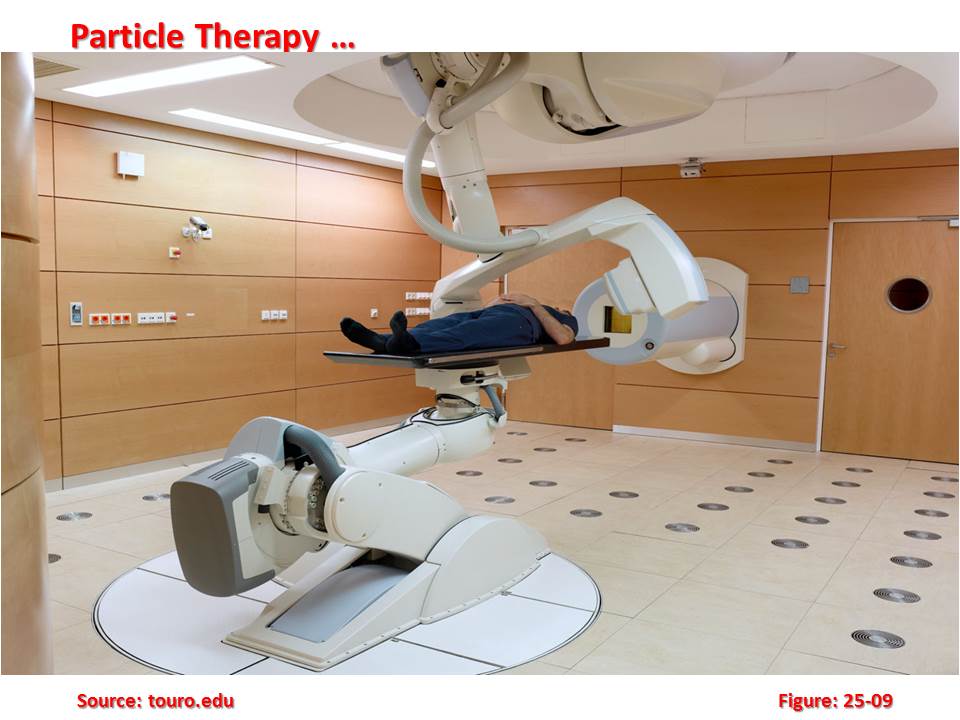 Particle therapy, which uses the properties of fast proton and ion beams, has already achieved initial clinical successes. Furthermore, a partnership between GSI and Siemens Medical Solutions is expected to set the stage for specialized clinical centers that guarantee patients a level of care that corresponds to their requirements. “The heightened release of energy by ions at the end of their trajectory through body tissue in conjunction with their high biological effectiveness makes them an outstanding tool for irradiating deep tumours,” explains Dr. Thomas Haberer, technical project manager for therapy at GSI.
Particle therapy, which uses the properties of fast proton and ion beams, has already achieved initial clinical successes. Furthermore, a partnership between GSI and Siemens Medical Solutions is expected to set the stage for specialized clinical centers that guarantee patients a level of care that corresponds to their requirements. “The heightened release of energy by ions at the end of their trajectory through body tissue in conjunction with their high biological effectiveness makes them an outstanding tool for irradiating deep tumours,” explains Dr. Thomas Haberer, technical project manager for therapy at GSI.
With some tumours, conventional treatment methods from surgical removal and chemotherapy to radiological treatment and combination therapies come up against biological limits. These limits can be malignant growths that are difficult to reach, for example, or that lie near critical organs, as with brain tumours and tumours at the base of the skull. Another field of application comprises soft-tissue sarcomas and prostate carcinomas, which are surrounded by sensitive tissues. For these conditions, particle therapy is a new and effective course of treatment.
Particle therapy takes less time than conventional radiation therapies. 20 minutes of preparation and five to ten minutes of irradiation for an average of 20 days are enough to achieve marked remission of tumours and prevent the growth of new tumourous tissue. In addition, the treatment puts patients under a minimum amount of strain. Those who held jobs were able to continue working during therapy. Apart from minor swelling of mucous membranes and reddening of the skin, there were hardly any side effects. These benefits are a result of the special biological effectiveness of ion beams.
GSI accelerator system and the planned system in Heidelberg are designed to make the most of the grid scanning process. Ions are created in a gas discharge and injected into a system consisting of a linear accelerator and a synchrotron ring. In the synchrotron, the particles move in a circular path at up to 50 percent of the speed of light. The synchrotron provides therapy stations with a pulsed particle beam of a precisely defined energy, focus and intensity, delivering portions that are metered-out, so to speak. The energy level determines penetration depth; the intensity determines the irradiance; and the focus determines the decrease in dosage in the surrounding healthy tissue. These parameters can be changed in an instant.
Before treatment, a computer tomogram measures the tumour to an accuracy of about 1 mm. Treatment planners then divide the tumour volume perpendicular to the beam axis, defining virtual sections 2 to 3 mm in thickness, which are then successively scanned with the ion beam. In the case of typical volumes of 0.5 l, the radiation parameters must be calculated for approximately 20,000 points. During treatment planning, a team of specialists selects the optimal settings from a pre-established library of focal characteristics and intensity levels, allowing precision treatment of even the most difficult tumours, such as those that have wrapped themselves around a healthy organ.
There is an increasing use of particle therapy in the field of radiation oncology with increasing focus on the application of proton beam therapy. According to data from the Particle Therapy Co-Operative Group, as of March 2010 there are 30 proton therapy centres in operation worldwide, and more than 67,000 patients have been treated with this therapy. The number of operating proton centres is projected to double in the near future.
The advantage of particle therapy, including proton therapy, is that the particle beam can provide a more precise dose distribution compared to photon beam (X-Ray) radiotherapy. A particle beam deposits its energy at a certain depth as a sharp energy peak called Bragg peak, releasing a much lower dose before and almost none after this peak. Thus, by manipulating this characteristic, particle therapy can yield better dose distributions than photon therapy, providing the therapeutic dose to the tumour while minimizing unnecessary doses to healthy tissues.
1.8 Proton Beam Therapy:
Conventional radiation therapy directs photons (X-rays) and electrons at tumours with the intent of eradicating the neoplastic tissue while preserving adjacent normal tissue. Radiation-induced damage to healthy tissue and second malignancies are always a concern, however, when administering radiation. Proton beam radiotherapy, one form of charged particle therapy, allows for excellent dose distributions, with the added benefit of no exit dose. These characteristics make this form of radiotherapy an excellent choice for the treatment of tumours located next to critical structures such as the spinal cord, eyes, and brain, as well as for paediatric malignancies.
Conventional radiation therapy, which utilizes photon (X-ray) beams, is frequently used in the locoregional treatment of cancer. Tumour control is achieved by radiation-induced damage to DNA, which ultimately causes tumour cell death. In vitro, even the most radioresistant cancers can be eliminated. In vivo, however, lethal tumour doses are not always achievable because of radiation-induced morbidity in normal tissues.
Initially, patients were being treated at facilities designed and constructed for basic high-energy physics research, often resulting in very cumbersome treatments, as the proton beams were limited to a fixed (often horizontal) position, which meant that the patient had to be moved to align the tumour on the trajectory of the beam. This technique was in contrast to the isocentric capabilities of the modern linear accelerator that rotates around a point in space and can effectively target any site in the body.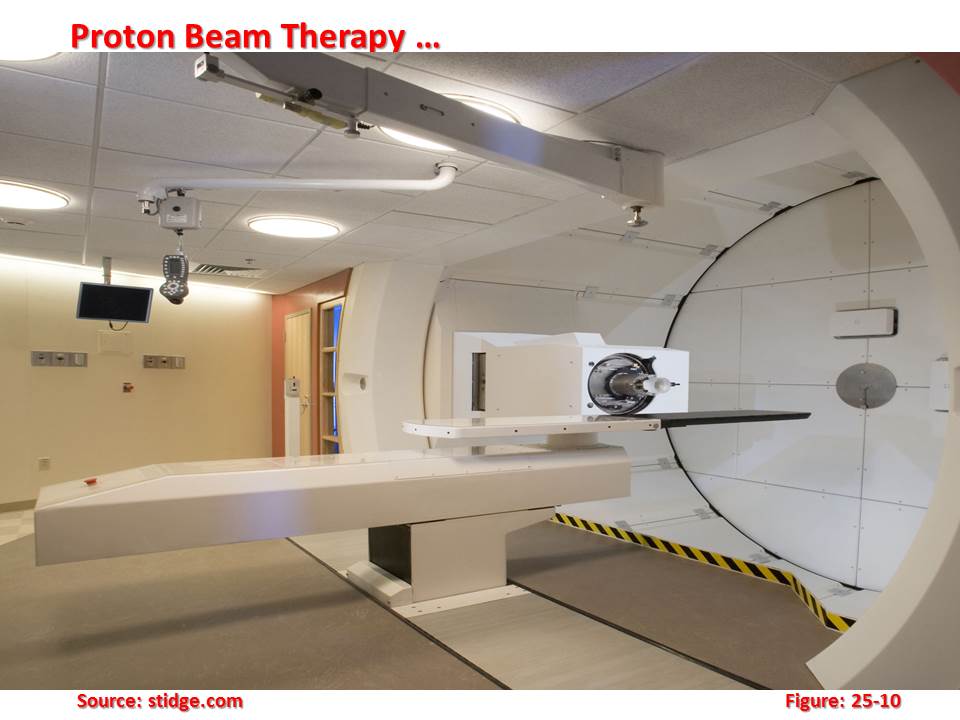 In addition, for many of the proton machines, the energy of the beam (which defined the depth of the Bragg peak) was only sufficient to treat superficial lesions (such as those of the eye) or intermediate-depth lesions (such as the base of skull). Owing to these technical factors and the interests of the involved physicians, the clinical sites that had initially received the most attention were uveal melanomas in the eye and base of skull sarcomas. The major emphasis for proton therapy clinical research initially was dose escalation for tumours adjacent to critical normal structures that constrained the doses that could be given with photons and for which local tumour control with conventional radiotherapy was thus poor.
In addition, for many of the proton machines, the energy of the beam (which defined the depth of the Bragg peak) was only sufficient to treat superficial lesions (such as those of the eye) or intermediate-depth lesions (such as the base of skull). Owing to these technical factors and the interests of the involved physicians, the clinical sites that had initially received the most attention were uveal melanomas in the eye and base of skull sarcomas. The major emphasis for proton therapy clinical research initially was dose escalation for tumours adjacent to critical normal structures that constrained the doses that could be given with photons and for which local tumour control with conventional radiotherapy was thus poor.
One of the pioneers in proton radiation therapy was the research facility at the Harvard Cyclotron Laboratory (HCL) in Cambridge, Massachusetts, operating in conjunction with the Massachusetts General Hospital. Patient treatment commenced in 1961 and ended in 2002, after the clinical programme was transferred to the Northeast Proton Therapy Center at Massachusetts General Hospital. In total, 9116 patients were treated at the HCL.
The development of hospital-based cyclotrons with higher energy beams capable of reaching deep-seated tumours (up to ~30 cm), field sizes comparable to linear accelerators, and rotational gantries have greatly facilitated proton radiation therapy. The first of these hospital-based facilities opened at Loma Linda University in California in 1990. Increasingly, there is interest in protocols aimed at morbidity reduction in those tumour sites in which tumour control with photons is good, such as many paediatric tumours.
1.9 Brachytherapy:
Brachytherapy is the administration of radiation therapy by placing radioactive sources adjacent to or into tumours or body cavities. With this mode of therapy, a high radiation dose can be delivered locally to the tumour with rapid dose fall-off in the surrounding normal tissues. In the past, brachytherapy was carried out mostly with radium or radon sources. Currently, the use of artificially produced radionuclides such as caesium-137, iridium-192, gold-198, iodine-125 and palladium-103 is rapidly increasing. According to the definition of the International Commission on Radiation Units (ICRU), high dose rate (HDR) brachytherapy means more than 12 gray per hour (Gy/h), although the usual dose rate delivered in current practices is about 100–300 Gy/h. The use of HDR brachytherapy has the advantage that treatments can be performed in a few minutes allowing them to be given in an outpatient setting with minimal risk of applicator movement and minimal patient discomfort. Remote controlled after loading brachytherapy devices eliminate the hazards of radiation exposure.
According to the definition of the International Commission on Radiation Units (ICRU), high dose rate (HDR) brachytherapy means more than 12 gray per hour (Gy/h), although the usual dose rate delivered in current practices is about 100–300 Gy/h. The use of HDR brachytherapy has the advantage that treatments can be performed in a few minutes allowing them to be given in an outpatient setting with minimal risk of applicator movement and minimal patient discomfort. Remote controlled after loading brachytherapy devices eliminate the hazards of radiation exposure.
A recent development in the field of HDR brachytherapy is the miniaturization of cobalt-60 sources into micro sources that are the same size as a HDR iridium-192 source. These new systems have the same versatility of all modern after loading HDR systems but with the added advantage of using an isotope with a half-life of 5.27 years. This makes it possible to replace the source only every 5 years instead of every 3–4 months, as is the case with iridium-192.
The savings in terms of resources, time and procedures are significant. Currently, the image-based treatment planning of gynaecological brachytherapy takes full advantage of modern imaging techniques (CT, MRI) to visualize the tumour, the applicators and the organs at risk and prescribes the doses accurately.
2. CONCLUSION:
The potential or actual use of new advanced technologies raises questions about cost, efficacy and ethics. The increased capital and operating costs and the economic burden of increased QA is a challenge. Stereotactic radiosurgery, stereotactic body radiation therapy (SBRT), proton and other charged particle therapies using single or hypo-fractionation regimens have the advantage of saving time but require well-qualified personnel and excellent QA/QC programmes, as there is little chance of adjustment once the treatment has been initiated.
The major challenges for using technically advanced equipment and techniques are:
- Appropriate human resources;
- Qualified and trained staff for the accurate delivery of high therapeutic radiation doses;
- Infrastructure requirements capable of handling this technology most efficiently and effectively;
- Types and stages of cancers to be treated;
- Development of commissioning and QA/QC protocols; and
- Institutional resources and clinical backup to deal with increased downtime for the more complex technologies.
Advanced technological needs for radiation oncology must be considered in the context of the needs of the countries concerned in terms of essential infrastructure in order to allow for a smooth, incremental and safe progression to advanced radiotherapy services.
An important theme echoed by experts is the global shortage of skilled professionals. It is noted that while short-term and local solutions have been devised, there is a need in many countries for a long-term strategy to establish training programmes and produce trainers and educators who could increase the availability of adequately trained staff in the radiotherapy disciplines. Training must be adapted to both the working environment and the available technology; a trainee or the trainee’s institution derives little benefit when the education addresses a technology not available in his or her own country.
There is clearly a role for networking on the national and regional levels to support local education programmes.
Resources:
- IAEA – Nuclear Technology Review;
- IAEA – Nuclear Energy Review – 2010;
- Radiology Information Organization;
- City of Hope;
- The British Journal of Radiology;
- NCBI;
- Siemens; and
- BJC – Proton Beam Therapy.
- This chapter was published on “Inuitech – Intuitech Technologies for Sustainability” on April 24, 2012; and
- This chapter was updated on 26 June 2020.
It is really a great and helpful piece of info. I’m glad that you simply shared this useful information with us. Please keep us informed like this. Thank you for sharing.